

RO-ILS Case Study 11
Pause for Concern: Adjacent Isocenters and Timeouts
Introduction
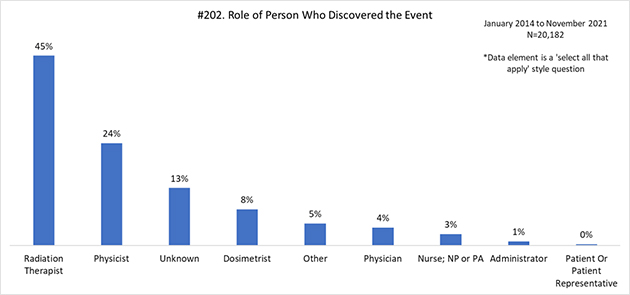
Radiation therapists play an important role in the safe delivery of radiation, especially given their ability to act as a final safety barrier. They perform the critical last safety checks (e.g., timeouts) before the administration of radiation and therefore must remain focused on the tasks at hand. As of November 2021, 45% of RO-ILS events were discovered by a radiation therapist. Their ability to stop errors from reaching the patient is dependent on voicing concerns and stopping treatment to address clinical needs. For this reason, radiation therapists must be empowered to speak up and halt processes. These same principles apply after an error has reached the patient.
An important underpinning of all clinical work is establishing a culture that enables collaboration and a prioritization of safety. As vital team members in the patient’s care, radiation therapists must work with their colleagues to establish a comprehensive culture of safety that places the patient’s safety as paramount to other clinic pressures.
Case Example
Overview: A patient receiving radiation treatment to the T-spine and L-spine, with two isocenters, was treated incorrectly. Accurate notes were not documented on the patient’s schedule and a comprehensive timeout was not performed. After the initial error, the therapists completed treatment without guidance from the physician or medical physicist, ultimately resulting in unintended dose being delivered to both sites.
Details:
- A patient was prescribed radiation treatment to the T-spine and L-spine.
- Two separate prescriptions and plans were created, with each site prescribed a total dose of 3750 cGy in 15 fractions.
- Notes on the patient’s schedule stated “spine” but did not specify multiple isocenters.
- On fraction 4, during setup of the T-spine, the therapist at the console was distracted by a phone call and opened an additional window in the oncology information system . This additional window obscured the correct treatment site.
- The 4-field L-spine prescription was selected instead of the T-spine.
- During the verbal timeout, “spine” was confirmed by the treating therapist.
- The AP field-1 of the L-spine prescription was delivered to the T-spine.
- The error was caught by the treating therapist upon competition of the AP L-spine field-1 to the T-spine.
- The therapy team unsuccessfully attempted to contact the lead therapist and the medical physicist. The radiation oncologist was not contacted concerning the treatment variance.
- After several attempts went unanswered, the therapy team decided to continue the patient’s treatment.
- The patient was repositioned for the L-spine and the remaining 3 fields (L-Spine fields 2-4) were delivered to the correct location.
- The patient was then positioned to the T-spine isocenter and all T-spine fields were subsequently delivered to the T-spine.
- The final result was an overdose to the T-spine and an underdose to the L-spine.
Contributing Factors
- Lack of specific, written documentation explaining multiple isocenters and detailed anatomical sites.
- Several distractions present including the telephone call and multiple screens opened during treatment.
- Lack of comprehensive and specific timeout.
- Availability of senior staff.
- Failure to make an informed decision during a high-pressure event.
Lessons Learned/Mitigation Strategies
- Treatment to adjacent isocenters should be handled with care.
There is added risk of errors with added complexity, including multiple treatment sites. Therefore, specific written set-up documentation should draw attention to this critical information. Additionally, couch tolerances may need to be adjusted to avoid treatment variances. Another method to minimize errors is to image one or both isocenters before the initiation of treatment. - Distractions should be minimized to avoid treatment errors.
Distractions during radiation therapy delivery are inevitable. The telephone is one of the main distractions to a radiation therapist. It’s important that the treating radiation therapist gives the patient their undivided attention and avoids all distractions while treating a patient. The practice’s culture must support staff in prioritizing the task at hand and discourage unnecessary multi-tasking. In the event of an emergency phone call, the treating therapist should step away from the console and allow another trained radiation therapist to complete the patient’s treatment. Also, additional screens obstructing the therapist view should not be opened while treating patients. - A comprehensive and specific timeout should be performed on all patients
All team members participating in the patient’s treatment should stop and acknowledge critical information (e.g., patient ID, treatment site(s), approved prescription, treatment accessories, imaging as needed). In the event there are multiple isocenters, more specificity must be included. Given the inherent collaborative nature of therapists’ work, they must communicate in a clear and specific manner with their colleagues, whether at the console or with the patient in the room. Radiation therapists, along with the entire team, are required to be accurate and precise, so it is imperative that staff remain vigilant and consistent. - Treatment should be terminated when an error occurs
In the event of a treatment variance, it is important to create a hard stop until all concerns are addressed. Practices should develop a protocol (e.g., call tree) so it is clear who is contacted when staff are unavailable and how to escalate urgent questions. For example, if questions arise, therapists should contact the lead therapist, dosimetrist, physicist, and ultimately, the treating physician regarding the variance to gather more input. Staff should not continue with the patient’s treatment until all parties agree on the plan of action. While the specific rationale for continuing treatment in this case is not known, it does highlight the importance of safety culture. Practices must promote a culture in which team members are comfortable reaching out to any staff member and are empowered to stop treatment until questions and issues are resolved. Discussing these types of safety events in staff training can be helpful to facilitate open dialogue and safety culture.
Safety Check
- Are all treating staff participating in a comprehensive time out (i.e., Correct patient? Correct site? Imaging orders?)?
- Are all staff comfortable posing safety questions, voicing concerns and pausing treatments until they are addressed? Is there a policy for a “hard stop”?
- How does your practice handle distractions at the treatment console?
