

Posted: July 1, 2026
Last fall, at the 67th Annual Meeting in San Francisco, two California-based organizations, Latinas Contra Cancer and Carter’s Foundation were each awarded the Survivor Circle Grant for $12,500. These two special organizations enthusiastically shared how they have used the grant to support their missions thus far.

ASTRO 2026: What’s New This Year
Posted: June 17, 2026ASTRO President Neha Vapiwala, MD, FASTRO, shares details on some of the new events and workshops at this year’s 2026 ASTRO Annual Meeting in Boston, September 26-30.

Honey, They're Sending Me to Kathmandu!
Posted: April 28, 2026Every time ASTRO staff reach out with a new APEx facility visit assignment, there's a familiar flurry. Pull up the clinic schedule, figure out which colleagues can cover, check flight options, debate whether to try for the red-eye home or spend another night. There's logistics. There's calendar Tetris. And honestly? There's always a little bit of jitters, a new facility, a new team, a new city, and a responsibility not taken lightly.
A Message from the CEO: The 2026 Reimbursement Crisis and ASTRO’s Response
Posted: April 21, 2026The first quarter of 2026 has brought significant financial instability and uncertainty for many in our field. The 2026 payment rules for both the Hospital Outpatient Prospective Payment System (OPPS) and, especially, the Medicare Physician Fee Schedule (MPFS) introduced numerous fundamental changes. While the full impact of these changes may take months or even longer to fully understand, the struggles faced by radiation oncologists and cancer centers are real and immediate — and merit immediate action.
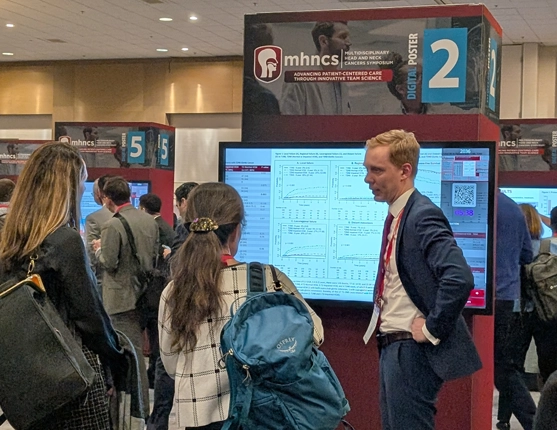
Couldn’t Make It to the Head and Neck Symposium in February? Here’s a Recap (+ onDemand access details)
Posted: April 7, 2026This year’s Multidisciplinary Head and Neck Cancers Symposium was dedicated to the theme of “Advancing Patient-centered Care through Innovative Team Science.” Held on February 19-21 in Palm Desert, California, the meeting brought together diverse voices across oncology disciplines. Dynamic sessions, plenaries, and poster presentations fostered conversations that navigated the complexity of H&N cancers with an integrated, collaborative mindset.
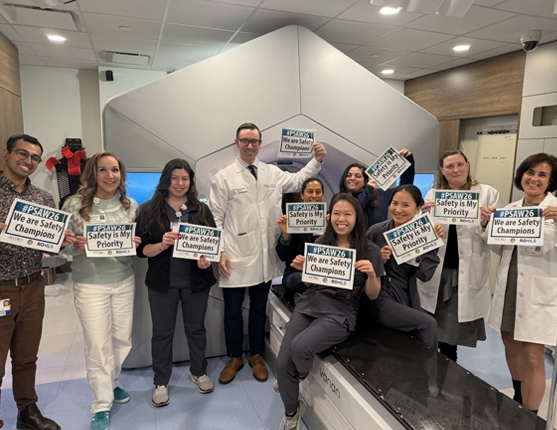
Patient Safety Awareness Week: Radiation Oncology’s Leadership in Safe Patient Care
Posted: March 9, 2026Patient Safety Awareness Week is an opportunity to reflect and spotlight our specialty’s commitment to always providing safe, high-quality care. In radiation oncology, safety is the foundation of our culture and woven into every treatment we deliver. Each radiation oncologist, medical physicist, dosimetrist, radiation therapist and staff member plays a key role in this mission.
DC Cancer Support Organizations Share Impact of Survivor Circle Grants
Posted: February 25, 2026Two Washington, DC-based organizations, Smith Center for Healing and the Arts and Touch4life, were selected in the fall of 2024 as ASTRO’s Survivor Circle grant winners, receiving $12,500 each. For over 20 years, the grant has been awarded annually to selected organizations for the services they provide to cancer patients, their families and caregivers, in the state hosting ASTRO’s Annual Meeting. Read more about how the grants deepened the impact of each organization and details on this year’s application.

Turning Copper into Care: How Two Dartmouth Therapists Sparked a Sustainable Giving Movement
Posted: December 10, 2025In radiation oncology, innovation often invokes advanced technologies, clinical trials and precision treatments. But sometimes, meaningful progress begins in the most unexpected places — like the back closet of a rural radiation oncology clinic in northern Vermont.
Expanding ASTRO’s Global Presence - Introducing the ASTRO International Ambassadorship Program
Posted: December 3, 2025ASTRO is pleased to announce the inaugural class of ASTRO International Ambassadors. Selected by the International Committee, these ambassadors are entrusted to represent ASTRO within their local communities and to spearhead national collaborative initiatives aimed at increasing visibility, supporting membership growth and facilitating strategic partnerships.

A Dose of Poetry
Posted: November 12, 2025What were you doing on the last day of the 2025 ASTRO Annual Meeting? Some of us decided once again to walk the streets of San Francisco, dodge Waymos, and gather at the conference center for one last hurrah — this time to discuss poetry. With fresh coffee, free books, and Red Journal swag, we met for “A Dose of Poetry: A Poetry Workshop Hosted by the Red Journal.”
