The Hodgkin Mixtapes
Benjin Facer, MD, is a 2025 graduate of The Ohio State University radiation oncology residency program and recently started community practice with Baptist Health based in Louisville, Kentucky. As a long-term survivor of pediatric Hodgkin lymphoma, Benjin has lived with the experience of his cancer diagnosis and sequelae of combined modality therapy for nearly his entire life.
A Mother’s Intuition
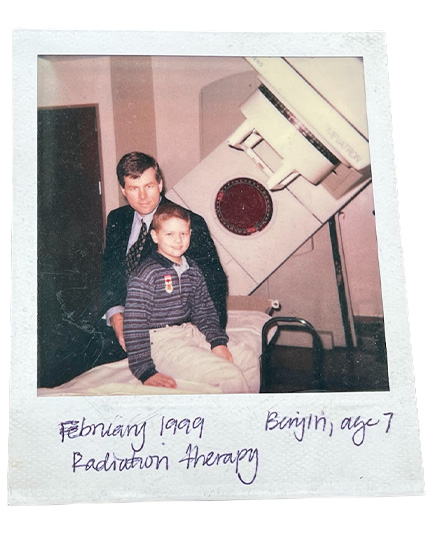
When he was 6 years old, Benjin and his four brothers — one of them a newborn — moved with their parents to Minnesota. In addition to struggling to adjust to a new environment and a new family member, he also started to feel ill almost all the time, often with a fever, for about six months. His doctors didn’t think much of his symptoms at the time, but his mother had a much higher index of suspicion that something was really wrong and pushed for answers.After a “diagnostic odyssey” involving lots of blood tests and scans and biopsies, Benjin was eventually diagnosed with a Stage IIIB classic Hodgkin lymphoma with bulky mediastinal involvement, cervical adenopathy and splenic involvement. Although not formally enrolled on a clinical trial, he was treated according to the Children's Cancer Group (CCG) 5942 protocol, which incorporated involved field radiation therapy to 21 Gy in 12 fractions.1
A growing literature in caregiver burnout shows just how widespread the effects of such a diagnosis and treatment can be, especially when the patient is in the pediatric age range.2 Benjin’s parents were his primary support system, but he distinctly remembers how so many good people of the Land of 10,000 Lakes, neighbors who had only recently met their family, stepped in to help without any prompting by watching his siblings, helping with housework and offering much-appreciated encouragement.
“The Kid with Cancer”
A few years ago, Benjin ran across a friend from elementary school on Facebook and decided to reach out. A jolting reply: “Oh, you were the kid with cancer!” Ouch.In retrospect, he realized that having cancer was likely his defining feature to his first-grade classmates, even though it was only a small part of who he felt he was. He notes, “I was bald at school and people probably looked at me a lot more than I realized. But I didn’t think of myself as a cancer patient; I thought of myself as a soccer or basketball player.”
Although Dr. Facer the budding radiation oncologist had expected that his own experiences might help him connect more easily with his patients, he quickly realized that each patient’s journey with cancer is unique and that trying to relate through his own cancer journey often missed the mark. “It’s not that my patients don’t care about my own personal cancer journey, but their story is their own. My experience as a 6-year-old was different than most adult patients I’m treating.” Instead, he tries to relate to patients with resources that were — and continue to be — helpful for him. Benjin notes that for some, support groups can be amazing. For others, they can be depressing, especially when the attendees span a wide spectrum of ages and prognoses. The key is finding resources that fit the patient. One program Benjin loves to promote is called First Descents.3 This non-profit organization hosts free, week-long outdoor adventures for young adult cancer survivors. These excursions, including rock climbing, kayaking and surfing, provide community and connection for people who are used to feeling different.
“Several of the participants on my First Descents trip talked about the psychological strain of looking around and only seeing 60-80-year-olds in the waiting room,” Benjin said. “But sometimes it’s also hard for young adults to fit in with peers who don’t understand their struggles. First Descents gives people a special week to have fun, relax and feel ‘normal’ again around people who are battling similar demons.” While programs like First Descents may not be a good fit for everyone, Benjin feels that we owe it to our patients to become informed about what’s available. “Different people are going to cope in different ways, so the best thing we can do is be knowledgeable about what’s out there, and make sure our patients are well-informed of their options.”
A Life-Saving Plan
Even as most of us will try to follow our patients for at least five years or so after treatment, this may not be enough, especially for pediatric patients. Benjin credits the Survivorship Care Plan from Vanderbilt Children’s Hospital for saving his life. His parents were educated about proper screening and made sure he always completed his surveillance imaging, including thyroid ultrasounds. Fifteen years after completion of therapy, a routine surveillance thyroid ultrasound detected a Stage I thyroid cancer, which was successfully resected.But for Benjin and many other childhood cancer survivors, a hazy future continues to be a source of concern. Well-deserved celebrations of improvements in cancer outcomes4 must be met with a stark awareness of possible, unanticipated long-term toxicities. Long-term side effects of treatment, including financial toxicity, are frequent challenges.
Benjin spent his research year during residency working for Nanobiotix, the creator of NBTXR3, a radioenhancing nanoparticle with the potential to escalate radiation dose to the tumor without harming surrounding tissue. But he would point out that for even the best innovation, be it a new technology or simply a new dosing regimen, we simply won’t have 30-year toxicity data. So, when should we dance with the devil we know, being mindful of the strides we’ve made in treatment planning and toxicity reduction, and when should we accept the unknown long-term toxicities of novel therapies?
Time will tell what future suffering we avoid or cause in this bargain. In the meantime, he believes, our field must strive for comprehensive accounting of long-term toxicities through initiatives like PENTEC.5 These efforts will help us recognize and counsel our patients about risks and benefits of our treatments, not just through year five, but for a lifetime.

Rewind
One core memory of his radiation therapy course sticks out. The treatment vault had a cassette player, and he was encouraged to bring in tapes to listen to during treatment. His parents asked his extended family to record something on a tape so Benjin could have something fun to listen to during his treatments. He comes from a large family, with dozens of cousins. Each family took a different tact; some sang songs, others told funny stories, and others just talked to him. Unfortunately, the cassette player malfunctioned before he started treatment, so he listened to them in the car on the way to and from treatment. “That was my pump-up music for treatment! I felt so much love from those tapes.”At the close of our conversation, Benjin was on his way out to an appointment — not for one of his patients, but one of his own surveillance appointments. Although our therapies and understanding of long-term toxicities have greatly improved in the 50 years after the seminal editorial of Guilio D’Angio, MD, the words still ring true – “indeed, cure is not enough.”6
Cars don’t have cassette players anymore, but while driving to see his doctor, Benjin can still hear in his head his cousins singing woefully off key, and it makes him smile.
References
- Wolden SL et al. Long-term results of CCG 5942: a randomized comparison of chemotherapy with and without radiotherapy for children with Hodgkin's lymphoma—a report from the Children's Oncology Group. J Clin Oncol. 2012 Sep 10;30(26):3174-80.
- Junkins CC et al. Cancer across the ages: a narrative review of caregiver burden for patients of all ages. J Psychosoc Oncol. 2020 Nov-Dec;38(6):782-798.
- First Descents. https://firstdescents.org/. Accessed November 14, 2025.
- Herrera AF, LeBlanc M, Castellino SM, et al. Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma. N Engl J Med. 2024;391(15):1379-1389.
- Pediatric Normal Tissue Effects in the Clinic. https://www.pentecradiation.org/. Accessed November 12, 2025.
- D'Angio GJ. Pediatric cancer in perspective: cure is not enough. Cancer. 1975 Mar;35(3 suppl):866-70.
