

RO-ILS Case Study 16
Prescription Transcription Error and Incorrect MUs
Download RO-ILS Case Study 16.
Introduction
Near misses offer a free learning opportunity if they are reported, reviewed and acted upon. The following RO-ILS case describes a calculation error that would have resulted in a sentinel event had it reached the patient. It highlights the potential for a transcription error to go undetected during the plan review process and the need to identify and enact effective mitigation strategies.
Event Overview
A patient was scheduled to have standard whole brain treatment. The intended prescription was 300 cGy x 10 fractions for a total of 3,000 cGy. However, there was a transcription error and an extra zero was entered into the treatment planning system (TPS). Therefore, the plan was calculated incorrectly for 3,000 cGy x 10 fractions for a total of 30,000 cGy and approved by the radiation oncologist.
During initial physics plan check, the physicist noted the unusually high monitor units (MU) for the treatment fields. Further investigation showed a maximum dose on dose volume histogram (DVH) of greater than 30,000 cGy. The error was corrected prior to the patient’s treatment.
The MU second check software did not flag this as an error as its results matched the TPS.
Contributing Factors
- Personnel
- A staff performance slip when entering the prescription dose in the TPS.
- Inadequate plan review by the dosimetrist and radiation oncologist, with failure to recognize the unusually large number of MUs per field and DVH absolute dose values.
- Environment
- The RO-ILS user indicated that this event occurred during an extreme weather event and identified rushing as a contributing factor.
- Technology
- Lack of adoption by software vendors of standardized prescription format.
- Lack of seamless interoperability between systems: MU second check software cannot confirm that calculated dose matches prescription dose.
Lessons Learned and Mitigation Strategies
1. Dosimetrists must review calculated MUs against a reasonable expectation of calculation result.
Beam calibration is usually done so that 1MU = 1cGy at the reference beam and measurement parameters. Therefore, it is a reasonable expectation that an unmodified beam (without wedge, compensator, fluence modulation, etc.) should have MUs approximately equal to the field dose. In this example, MUs for each field should be close to 150 MU based on the prescription. Highly modulated VMAT/IMRT fields will tend to have higher MUs than less modulated fields. Wedged fields will have higher MUs than open fields with the same weight, etc. Such sanity checks are essential during finalizing a plan and during its review, so that oversights such as the present case can be prevented.
2. Physicist and physician review must include verification that treatment plan matches intended prescription dose/fractionation.
Potential aids to this review are:
- Physician plan approval should be standardized; for instance, according to the CB-CHOP format1 which stipulates a review of the prescribed dose.
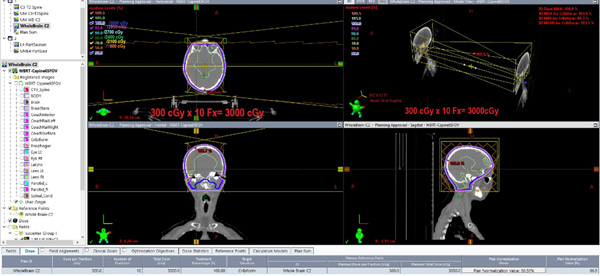
- Review plans in absolute dose. This error would have been immediately discovered had absolute dose been reviewed. Vendors could support this by enabling easy review of plans in absolute and relative dose during plan review (Figure 1).
- Prescription display as part of the main isodose review window, rather than a separate tab, would be useful in assessing similar errors (Figure 1).
Prescribed dose is in the bottom of axial and BEV windows in the proposed 2016 white paper format. Additionally, both relative and absolute doses are keyed simultaneously in the upper left-hand corner of the axial display.
3. The radiation oncology community should use the standardized prescription format uniformly.
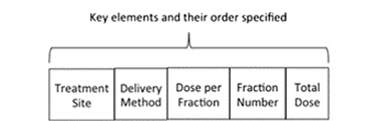
The accurate, timely, unambiguous communication of the radiation prescription is a critical part of the radiation planning and delivery process. Standardization facilitates this clear communication. Standardizing dose prescriptions: An ASTRO white paper2 provides the key elements (Figure 2), units (e.g., dose in cGy), rationale for standardizing prescriptions, and challenges to standardization. The specialty needs to address barriers and work toward complete adoption of a standardized prescription order and units by everyone – this includes clinicians in everyday work, presentations, studies/scientific articles, and software vendors.
4. Second MU check software could be improved to evaluate if the second check calculation results are reasonable for the prescription.
This could take the form of the software reading the prescription from the DICOM data and comparing it to the calculated MUs or forcing an entry of the prescription and comparison of the second check calculation to that.
5. Facilities could identify additional mitigation strategies to confirm that prescription data in the TPS matches an expected prescription dose/fractionation.
Humans are fallible and therefore typos and errors will happen. Increased vigilance of commonly used prescriptions can be helpful; however, awareness and the suggestion to be more careful is low on the hierarchy of effectiveness. Therefore, it can only be a first step and means of working toward and advocating for more effective solutions. For example, this may include reviewing and confirming that software MU limits are set and reasonable to help catch errors. To reduce the likelihood of typos, a practice may be able to reduce the need to type the information. Pre-defined planning templates that are selected or loaded automatically into the TPS could help avoid a data entry issue altogether.
Conclusion
This event demonstrates how a typo can lead to a potentially fatal overdose. While diligent quality assurance caught this error, and the multiple methods of plan review suggested in this report may have caught the error, there is significant potential for patient harm with errors of this nature. Of data reviewed between 2014 and 2016, one of the three common errors found in high priority RO-ILS events was “problematic plan approved for treatment.”3 This event falls into a subcategory of dose and fraction patterns being incorrect. This error pathway can take many forms but still exists and requires more attention. Facilities need to continue to enhance their quality assurance procedures. Planning software and second check software vendors can do more to help prevent and detect such errors.
Additionally, this event exemplifies the value of reporting near misses. A recent single institution study found different willingness-to-report scores for different types of near miss events, suggesting this may be due to the influence of cognitive biases in identifying what is worth reporting.4 Highlighting near misses is one way to demonstrate the importance of reporting them to RO-ILS so that the learning can be shared and disseminated to the broader community.
Safety Check
What processes are in place at your facility to ensure that the prescription is accurately entered into the treatment planning system? What checks do you have in your facility to confirm the calculated MUs are reasonable, given the technique? How does your facility promote near misses?
References
- Dean M, Jimenez R, Mellon E, et al. CB-CHOP: A simple acronym for evaluating a radiation treatment plan. Appl Radiat Oncol. 2017:28-30.
- Evans SB, Fraass BA, Berner P, et al. Standardizing dose prescriptions: An ASTRO white paper. Pract Radiat Oncol. 2016;6(6):e369-e381.
- Ezzell G, Chera B, Dicker A, et al. Common error pathways seen in the RO-ILS data that demonstrate opportunities for improving treatment safety. Pract Radiat Oncol. 2018;8(2):123-132.
- Kundu P, Jung OS, Valle LF, et al. Missing the Near Miss: Recognizing Valuable Learning Opportunities in Radiation Oncology. Pract Radiat Oncol. 2021;11(3):e256-62.
