

Case Study 15
Brachytherapy Applicator Digitalization
Download RO-ILS Case Study 15.Introduction
Brachytherapy requires specialized equipment, facility setup, process controls and staff who maintain competencies with the necessary specialized skills. A recent survey of radiation oncology residency graduates found that even though nearly all (97%) participants view brachytherapy as an important skill to develop during residency, only 54% expressed confidence in their ability to develop a brachytherapy practice post-residency.1 Because of the nature of high doses over one or a small number of fractions during brachytherapy treatment, it is especially important to identify and correct critical errors prior to treatment. These factors all makes brachytherapy a ripe area for learning from incident reports.
As of February 1, 2023, brachytherapy events comprised 2.3% of the events with known treatment techniques; the vast majority of which are related to HDR treatment (89%). Much can still be learned from previous RO-ILS education as well as historic foundational documents, such as AAPM report TG-59.2 RO-ILS has previously released education about brachytherapy events; for example, RO-ILS Quarter 3/4 2018 Report shared errors related to applicator reconstruction and treatment planning length measurements. This case study discusses a recent severe brachytherapy event reported to RO-ILS.
Event overview
Several patients who received brachytherapy treatment presented with unexpected skin reactions and the practice notified their radiation safety office. Upon subsequent investigation, they found additional patients with a similar adverse reaction. Patients who received treatment to one of two anatomical sites were affected by the error. It was determined that treatment was delivered at the connector end of the applicator instead of the tip end. The root cause of this event was the incorrect digitization of the applicator.
Contributing factors
- Lack of appropriate training and monitoring of competencies of staff members for special procedures.
- Inadequate policies and procedures in place for verifying the correctness of the digitization of the applicators.
Lessons learned/mitigation strategies
1. Initial training and competency evaluation for staff is essential for the various tasks they will be asked to perform, especially as it relates to brachytherapy procedures.
AAPM report TG-59 includes recommended training schedules for all staff, including medical physicists, involved in an HDR procedure. The process of digitizing a brachytherapy applicator is a critical step in the process and a variety of errors can occur during this step.3 Correct identification of the distal and proximal ends of the catheter is imperative during the digitization process.
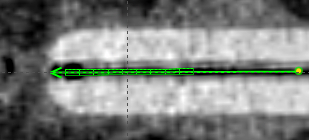
Figure 1: Treatment planning scan with digitization of the applicator
Furthermore, a clear distinction must be made between initial training and ongoing verification of competency. A 2016 AAPM subcommittee report offers a framework for practices to develop a credentialing and competency evaluation program.4 It emphasizes the importance of not only initial credentialing but also ongoing assessment of competencies for the various tasks that medical physicists are asked to perform. Additionally, it describes the differences between being board certified (having the appropriate credentials for a job) and credentialing and training to perform a specific task.
2. Pre-treatment chart checks must be developed to catch critical errors that could occur during the brachytherapy planning process.
AAPM report TG-59 reviews the entire brachytherapy process from simulation to treatment planning and delivery. It provides detailed HDR procedures for staffing, treatment-specific quality assurance and emergency procedures. Included in the treatment-specific quality assurance section, a list of checks should be done during the pre-treatment review of the HDR plan, including application digitization. It recommends that multiple staff members verify both the correctness of the applicator digitization and the correct length of the applicators. Moreover, a second independent review of the digitized applicator is essential during the plan review process. The document includes a workflow for both a one physicist and two physicist model in the staffing section and outlines the various responsibilities. In the event there is only one physicist, the treatment planner should perform the digitization so it can be double checked by the physicist; alternatively, both the task and quality check are performed by different physicists if multiple physicists are available. Another helpful resource is AAPM Medical Physics Practice Guideline 11a on brachytherapy plan and chart review.5 With specialized treatments like brachytherapy, practices must plan ahead and identify what the safest workflow would be if staff are unexpectedly not available (e.g., illness, emergency). Using a standardized checklist helps both experienced staff confirm all tasks are completed and is also an important tool for less experienced staff who may be filling in for unavailable staff.6
3. Risk analysis should be performed to improve policies and procedures and help mitigate the most harmful events from occurring.
AAPM reports are not meant to be taken as prescriptive documents. It is important that practices develop policies and procedures based on their workflow that are clearly documented and available to all staff for reference. The AAPM report TG-100 outlines a prospective approach to quality assurance and developing policies and procedures.7 It describes a method for a practice to develop process maps and fault trees to identify failure modes (errors) and rank them according to their severity and risk priority number. Upon identifying these potential errors, the practice can put into place safety barriers to prevent these errors from occurring in the clinic. It should be emphasized that this process is used to identify and prevent the most severe errors from occurring.
Conclusion
HDR brachytherapy applicator errors are not new. An analysis of NRC events over the course of two years found the most common error related to a misused applicator that resulted in the wrong site or wrong dose (a total of 11 events) was due to measuring the applicator length incorrectly or incorrectly entering the length in the treatment planning system.8 This case study demonstrates that the error pathways identified a decade ago still exist.
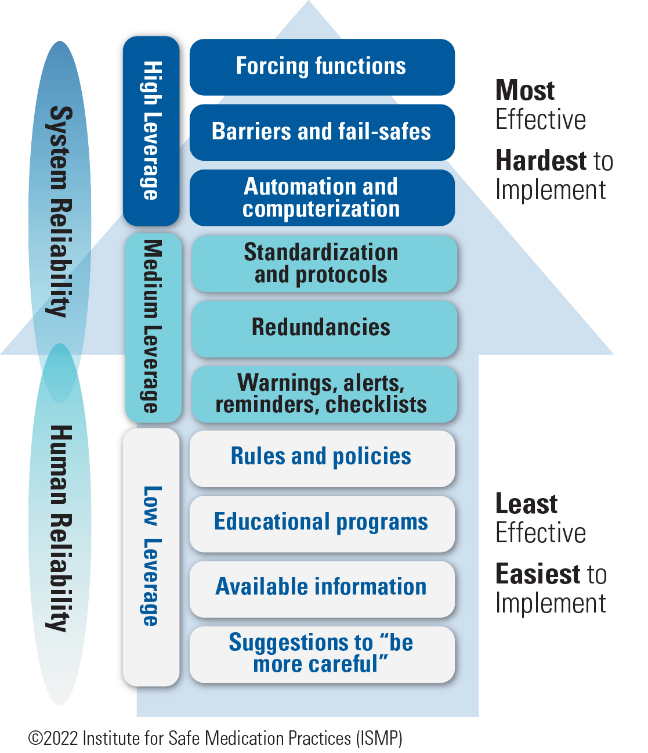
Figure 2: Hierarchy of Effectiveness9
Additional design elements (e.g., clear visualization and marking on applicators) and advancements that would be higher on the hierarchy of effectiveness (Figure 29) need to be further explored. For example, researchers are exploring the possibility of automating applicator digitization,10,11 which will require partnership and eventually implementation by vendors. More work needs to be done in the area of brachytherapy applicators and digitalization so that a decade from now, this error pathway is no longer possible.
Safety check
How are staff at your facility trained on digitalizing brachytherapy applicators and what checks and redundancies are in place to confirm it is accurately completed?
References
- Marcom SR, Kahn KM, Colbert LE, et al. Brachytherapy Training Survey of Radiation Oncology Residents. Int J Radiat Oncol Biol Phys. 2019;103(3):557-560.
- Kubo HD, Glasgow GP, Pethel TD, et al. High dose-rate brachytherapy treatment delivery: Report of the AAPM Radiation Therapy Committee Task Group No. 59. Med Phys. 1998;25(4):375-403.
- Wang K, Ferenci MS, de la Zerda A, et al. A review of nonstandardized applicators digitization in Nucletron™ HDR procedures. J Appl Clin Med Phys. 2017;18(5):89-96.
- Pavord DC, Birnbaum S, Bocuzzi D, et al. A report from the AAPM Subcommittee on Guidelines for Competency Evaluation for Clinical Medical Physicists in Radiation Oncology. J Appl Clin Med Phys. 2016 Jul 8;17(4):3-14.
- Xia P, Sintay BJ, Colussi VC, et al. Medical Physics Practice Guideline (MPPG) 11.a: Plan and chart review in external beam radiotherapy and brachytherapy. J Appl Clin Med Phys. 2021 Sep;22(9):4-19.
- Fong de Los Santos LE, Evans S, Ford EC, et al. Medical Physics Practice Guideline 4.a: Development, implementation, use and maintenance of safety checklists. J Appl Clin Med Phys. 2015 May 8;16(3):5431.
- Huq MS, Fraass BA, Dunscombe PB, et al. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Med Phys. 2016;43(7):4209.
- Richardson S. A 2-year review of recent Nuclear Regulatory Commission events: What errors occur in the modern brachytherapy era? Prat Radiat Oncol. 2012; 2(3):157-163.
- Education is “predictably disappointing” and should never be relied upon alone to improve safety. Institute For Safe Medication Practices. April 18, 2022. Accessed May 8, 2023. https://www.ismp.org/resources/education-predictably-disappointing-and-should-never-be-relied-upon-alone-improve-safety.
- Deufel CL, Tian S, Yan BB, et al. Automated applicator digitization for high-dose-rate cervix brachytherapy using image thresholding and density-based clustering. Brachytherapy. 2020 Jan-Feb;19(1):111-118.
- Yung H, Gonzalez Y, Shen C, et al. Deep-learning-assisted automatic digitization of applicators in 3D CT image-based high-dose-rate brachytherapy of gynecological cancer. Brachytherapy. 2019 Nov-Dec;18(6):841-851.
